

Hassan Kamal
Galilee Medical Center, Israel
Title: The impact of peritoneal glucose load on blood pressure in peritoneal dialysis patients
Biography
Biography: Hassan Kamal
Abstract
Background: Hypertension is considered well-known independent risk factors for cardiovascular morbidity and mortality in peritoneal dialysis (PD) patients. Cardiovascular complications are the main cause of morbidity and mortality in patients with end-stage renal disease and dialysis patients. Peritoneal glucose load (PGL) contributes to the development of cumulative peritoneal membrane damage and increased permeability, leading to fluid accumulation and elevated blood pressure.
The effects of PGL on hydration status, systemic inflammation, left ventricular mass, depression and male sexual dysfunction among PD patients was evaluated in our peritoneal unit in several prospective cross sectional studies conducted in the last 5 years (2014-2018).The relationship between PGL and blood pressure was not investigated before. Based on the data obtained from the mentioned studies and additional data that received from the usual maintenance follow up visits we evaluated retrospectively the influence of PGL on blood pressure in patients on maintenance PD.
Methods: Office blood pressure measurements were used. If white coat hypertension is suspected, a 24 hour blood pressure study was performed to assess the patient's overall blood pressure profile using Mobil-O-Graph device for 24-hour ambulatory blood pressure monitoring (Manufacture: Industrielle Entwicklung Medizintechnik GmbH, D-52222 Stolberg, Germany). The hydration status was assessed by a whole-body bioimpedance technique (BIS) using a Fresenius Medical Care Body Composition Monitor (BCM) device (Fresenius Medical Care, Bad Homburg, Germany). The PGL was assessed by PGL index (PGLI), which refers to the net glucose content (monohydrated or unhydrated) (g) in the PD solutions administered in the daily PD prescription divided by the dry body weight (kg) assessed by BIS:

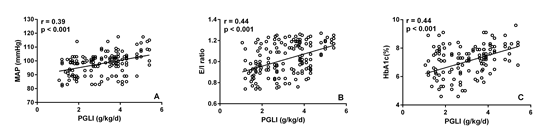
Results: One hundred fifty nine medical records of stable PD patients were evaluated retrospectively. Significant positive correlations were found between PGLI and mean arterial preasure (MAP), extracellular water (ECW)/ intracellular water (ICW) ratio and HbA1c. MAP, ECW/ ICW ratio and HbA1c were significantly higher in patients with PGLI > 3g/kg/day compared with those with PGLI ≤ 3g/kg/day.
Conclusions: PGL may be associated with higher blood pressure, overhydration and poor glycaemic control in PD patients. PGLI could be applied in managing PD patients as a practical tool for the quantitative assessment of the PGL. PGLI values bellow 3 g/kg/day should be targeted.
|
p |
Patients with PGLI > 3 g/kg/day n=76 |
Patients with PGLI > 3 g/kg/day n=83 |
|
|
<0.001 |
95.3±6.8 |
100.4±7.9 |
MAP (mmHg) |
|
<0.001 |
0.964±0.144 |
1.072±0.136 |
E/I ratio |
|
<0.001 |
6.56±1.13 |
7.52±0.94 |
HbA1c (%) |